Introduction
The perception we have of the world around us (including significant life events such as illness) results from our knowledge and experience, but also from the sociocultural environment (Vargas-Huicochea & Huicochea-Gomez, 2007; Vargas-Huicochea & Berenzon-Gorn, 2013). An array of socialization processes contribute to the development of relations that endorse or reject certain values or identities (Ellemers, Spears & Doosje, 2002), many of which may lead to stigmatizing or discriminating certain people. According to psychosocial models, stigma is based on a combination of three factors: lack of knowledge about a person’s condition (ignorance); development of negative attitudes (prejudice) and a tendency to exclude or reject certain individuals (discrimination) (Corrigan, 2005; Rose, Thornicroft, Pinfold & Kassam, 2007).
The general public’s concepts of severe mental illnesses such as schizophrenia or bipolar disorder are often based on myths and misconceptions. According to these stereotypes, individuals with a mental illness are unable to make appropriate decisions and are aggressive or dangerous to themselves and/or to the public (Link, Phelan, Bresnahan, Stueve & Pescosolido, 1999; Nedopil, 1997; Walsh, Buchanan & Fahy, 2002). Stigmatizing has a direct impact on patients’ timely diagnostic interventions and specialized treatments, which are frequently delayed in individuals who have been stigmatized (Sirey et al., 2001).
Providing more accurate information on multi-causality and the integral treatment of these problems together with objective information on the presence of aggressive behaviors could decrease the growing perception of the dangerousness of persons with mental illness, and should be complemented by the implementation of interventions to modify and eliminate misconceptions about the latter.
Mental Health Literacy (MHL), defined as the knowledge and beliefs about mental disorders that serve to improve their recognition, management, and prevention, also includes the ability to recognize certain mental illnesses and judge the comparative usefulness of a variety of interventions (Jorm, 2000; Yeo et al., 2001). Although one might expect stigmatizing attitudes to be more prevalent among persons with low educational attainment, several studies have shown that they are also common among many health professionals, including those who work with individuals with mental illnesses (Bolton, 2001; Fernando, Deane & McLeod, 2010). As gatekeepers to the health care system, medical professionals play a critical role in determining the impact of stigma on the quality of life of individuals with mental illnesses. Therefore, recognizing the presence of negative attitudes and identifying knowledge gaps in mental disorders among doctors and medical students constitutes the first step toward solving these problems.
In keeping with this theoretical framework, the main objectives of this study were to: 1. compare how undergraduate medical students evaluate certain aspects of MHL (illness recognition and suggested treatment) regarding bipolar disorder and schizophrenia. 2. determine whether there are differences in how they perceive aggressiveness and dangerousness in individuals with bipolar disorder and schizophrenia and 3. identify students’ attitudes toward these illnesses according to their perception of aggressiveness and dangerousness in both diagnoses.
Method
Study design
This is a non-experimental, comparative, cross-sectional study.
Participants
Sample size was determined with the Spiegel & Stephens formula (2009) since the distribution of the phenomenon related to the perception of aggressiveness-dangerousness was unknown. Therefore, a sample size of 98 was estimated with a confidence interval of 95% and a 10% alpha error.
Recruitment was performed by a cluster sampling approach with volunteer undergraduate medical students from a public university in Mexico City. Due to accessibility, for the present study researchers had access to two groups of medical students who were at the end of their first year of their degree course, when they had finished the classes of the subject in mental health offered in that school year. All students attending both groups were eligible to participate and there were no exclusion criteria, no incentives were included for participation, and there were no penalties for refusing to participate. After a verbal explanation of the aims of the study by one of the researchers, all students verbally accepted to participate voluntarily and the research questionnaire was completed within the context of the classroom and under the presence of the researcher if any doubt arose with regard to the questionnaire.
Assessment procedures
Public Conception of Aggressiveness Questionnaire
This questionnaire (Fresán, Robles-García, de Benito, Saracco & Escamilla, 2010) was used to assess mental illness recognition, beliefs about adequate treatment, and perception of patients’ aggressiveness and dangerousness. Like many studies in this field (Lauber, Nordt, Falcato & Rössler, 2003), the questionnaire was based on case vignettes. For the present study, two vignettes were written in a format to meet DSM-IV criteria for paranoid schizophrenia and bipolar disorder. The case vignette for schizophrenia was as follows:
This person is 25 years old. Until a year ago, life was ok but then things started to change. This person thought that people around were saying bad things about him/her behind his/her back. This person was convinced that people were spying on him/her and that they could hear what he/she was thinking. Eventually, this person could no longer work as a result of these thoughts, and spent most of the time in his/her room. This person heard voices even though there was no-one around. These voices told him/her what to do and think. This person has been living like this for six months.
The case vignette for bipolar disorder was:
This is a 22 year old who lives with his/her parents. Since a teenager, this person has been an athlete, with good grades and an adequate social life and has always sought new challenges. Occasionally, this person suffers from low mood lack of energy that does not affect his/her functionality. This person is in the last semester of his/her degree program in architecture and academic pressure has recently increased. In the past three weeks, his/her parents and friends have noticed that this person talks too fast, is irritable, skips classes and fails to complete assignments. Some school colleagues have said, “Something is happening to his/her behavior, and sometimes he/she talks nonsense”. His/her parents were surprised because he/she has never been a problem, but two nights ago, this person took his/her mother’s car without permission and returned it with a dent that didn’t explain. This person has also had practically no sleep for nearly four days. This person says that nothing is wrong and that feels better than ever, that is not going to school because he/she doesn’t need it because classes are boring and that he/she could actually teach the professors a thing or two. He/she even says that he/she was called from the United States to teach a course.
Perception of aggressiveness and dangerousness
Patients’ level of aggressiveness was assessed through four questions to evaluate perception of: 1. Verbal aggression, 2. physical self-aggression, 3. physical aggression against objects, and 4. physical aggression against others. Each of these questions has five levels of severity to classify aggressive behavior. For example, verbal aggression includes behavior ranging from no verbal aggression (rated as 0), through shouting angrily (rated as 2) to making clear threats of violence towards others or the subject himself (rated as 4). The following item was used to assess perception of dangerousness: “I think this person is a dangerous person for society”, which was rated on a 4-point Likert scale from strongly agree to strongly disagree.
Mental illness recognition and beliefs about adequate treatment
For both vignettes, respondents were asked to consider whether the person described in each of them had a mental illness, which was also rated on a 4-point Likert scale from strongly agree to strongly disagree. Regarding their perception of what they considered the most adequate treatment, several options were included and students should select the one they consider most appropriate. For analysis purposes and results presentation, treatment options were ranked according to the level of restriction: 1. non-psychiatric, non-restrictive intervention (e.g., talking to the person or closer observation), 2. psychiatric intervention (e.g., use of oral medication, injections or hospitalization), and 3. restrictive intervention (e.g., seclusion, use of restraints or treatment for injuries).
The Public Conception of Aggressiveness Questionnaire has shown an adequate internal consistency (general Cronbach’s alpha = .74) as well as construct validity (explained variance = 61%) (Fresán et al., 2010) and has been previously used in the assessment of schizophrenia (Fresán et al., 2010; Robles-García, Fresán, Berlanga & Martínez, 2013) and bipolar disorder (Fresán, Berlanga, Robles-García, Álvarez-Icaza & Vargas-Huicochea, 2013).
The Opinions about Mental Illness Scale (OMI)
The OMI was used to evaluate personal attitudes toward persons with severe mental illness. The OMI is a 34-item self-report questionnaire that evaluates these attitudes utilizing a 5 -point Likert scale (1 = totally disagree; 5 = totally agree). Evaluation includes six factors: 1. separatism (score range 10 - 50), which emphasizes a person’s perceived differences about a mental disorder and the desire to keep his distance in order to be safe; 2. stereotyping (score range 4 - 20), defined as regarding mentally ill persons in keeping with certain behavioral and intellectual patterns; 3. restrictiveness (score range 4 - 20), which includes items that support an unclear notion of the rights of mentally ill persons; 4. benevolence (score range 8 - 40), which evaluates compassion towards the mentally ill; 5. pessimistic prediction (score range 4 - 20), the belief that mentally ill persons are incapable of improving their symptoms and society’s lack of optimism in this respect; 6. stigmatization (score range 4 - 20), comprising items that perceive mental illness as a reason for shame (Fresán et al., 2012; Ng & Chan, 2000). Internal consistency of the OMI in Mexican population was adequate (Cronbach’s alpha = .77) (Fresán et al., 2012).
Statistical analyses
Demographic and clinical characteristics were analyzed with frequencies and percentages in the case of categorical variables and with means and standard deviations (S.D.) when presented as continuous variables. McNemar tests were used for nominal data and applied to 2 × 2 contingency tables to determine marginal homogeneity regarding the perception of the presence of aggressiveness, dangerousness and mental illness recognition through bipolar and schizophrenia vignettes in undergraduate medical students. For this analysis, items related to perception of aggression were dichotomized as absent or present (all four intensity levels), while items rated on a 4-point Likert scale were dichotomized as agreement (strongly agree and agree) and disagreement (strongly disagree and disagree) to perform percentage comparisons. Attitudes toward persons with severe mental illness (OMI scales) according to perception of aggressiveness and dangerousness for both diagnoses were compared using independent sample t-tests. All tests were two-sided with a significance level of p ≤ .05. We analyzed our data using the statistical software package SPSS, version 16.0, for Windows P.C.
Ethical considerations
Informed consent was obtained from all the individual participants included in the study, who received no remuneration for their participation. Both the Ethics Review Board of a specialized psychiatric institution and the university authorities approved the study, which is in accordance with the Helsinki Declaration of 1975 (World Medical Association, 2013).
Results
A total of 104 medical students in the first year of their degree course participated. Seventy-one of them were men (68.3%) and the remaining 33 (31.7%) women, with a mean age of 18.8 (S.D. = 1.9) years.
Mental illness recognition and beliefs about adequate treatment
Only 36.5% (n = 38) of the total sample identified the presence of a mental illness in the subjects described in both clinical vignettes; however, more medical students identified a mental disorder in the schizophrenia (n = 57, 54.8%) than the bipolarity vignette. Only four students (3.8%) considered the opposite condition, bipolarity rather than schizophrenia, as a mental illness, and lastly, five students (4.8%) failed to see either the schizophrenia or the bipolarity vignette as a description of a mental illness (χ2 = 44.3, p < .001).
Psychiatric intervention for the schizophrenia vignette and non-psychiatric intervention (such as talking or closer observation) in the bipolar vignette were the options most frequently considered by most medical students (n = 61, 58.7%). A significant number of students considered that non-psychiatric intervention was the most useful intervention (n = 24, 23.1%) and only 7.7% (n = 8) considered psychiatric interventions (medication or hospitalization) for both diagnoses. Restrictive interventions (such as seclusion, use of restraints or treatment for injuries) was only considered for the schizophrenia vignette (n = 7, 6.8%) (Z = -7.3, p < .001).
Perception of patient’s aggressiveness and dangerousness
Although no information on specific aggressive behaviors was included in the vignettes, 75% (n = 78) of the medical students believed that the people described would eventually behave aggressively; while 10.6% (n = 11) considered that only the person in the schizophrenia vignette would behave aggressively, and 8.7% (n = 9) thought that only the person in the bipolarity vignette would do so, with no significant differences between the two (χ2 = .08, p = .82).
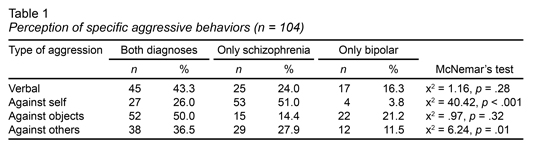
Nevertheless, when the perception of aggressiveness was assessed according to its behavioral manifestation, a higher proportion of medical students perceived self-aggressive behaviors (p < .001) and aggression against others (p = .02) in the schizophrenia vignette in comparison with the bipolar vignette, with no differences in terms of verbal aggression (p = .28) or aggression towards objects (p = .32) (Table 1). Similarly, perceived severity of aggressive behaviors was higher for the schizophrenia than the bipolarity vignette, with the following mean values (± S.D.): verbal aggression 2.39 ± 1.9 vs. 1.73 ± .65 (Z = -3.6, p < .001); aggression against self 1.86 ± .91 vs. 1.48 ± .67 (Z = 2.9, p = .003); aggression against objects 2.22 ± .81 vs. 1.30 ± .63 (Z = -5.5, p < .001) and aggression against others 1.84 ± .96 vs. 1.26 ± .44 (Z = -3.4, p < .001).
Dangerousness was more frequently perceived in the schizophrenia than in the bipolarity vignette (n = 7, 6.7% vs. n = 39, 37.5%, respectively), and even more so when both vignettes were considered (n = 28, 26.9%) (χ2 = 20.8, p < .001).
Attitudes toward persons with severe mental illness by perception of aggressiveness and dangerousness in schizophrenia and bipolar disorder
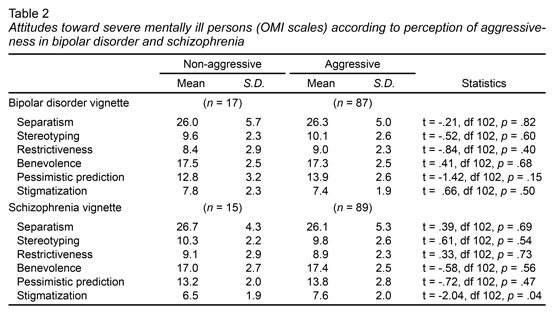
No differences emerged in attitudes toward the person described in the bipolar vignette according to the medical students’ perception of aggression. Nevertheless, more stigmatization was found among students who perceived aggression in the subject described in the schizophrenia vignette than among those who did not perceive aggressiveness in this person (Table 2).
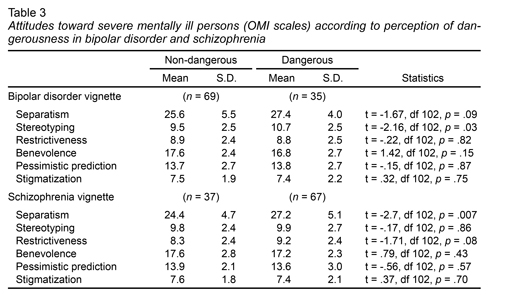
With respect to the perception of dangerousness, students who perceived it in the bipolar vignette expressed more stereotypical attitudes than those who did not perceive dangerousness. Regarding the schizophrenia vignette, students reported more separatism attitudes when dangerousness was perceived (Table 3).
Discussion and conclusion
Improvement of perceptions, attitudes, and treatments for psychiatric disorders is a constant concern among clinicians. Accordingly, one of the areas on which psychosocial research has focused is stigma towards mental illness. Although various strategies have been implemented to reduce both negative perceptions and attitudes towards persons with mental illness, they are insufficient, with misconceptions about these pathologies continuing to prevail.
Since health care professionals look after the sick (including psychiatric patients), it is essential for the treatment of these patients not to be biased by a lack of knowledge or prejudice towards psychopathology. Regarding mental illness, there is consistent evidence that physicians have similar perceptions to those of the general population and that these are not always positive (The Royal College of Psychiatrists, The Royal College of Physicians of London and The British Medical Association, 2001; Malhi et al., 2003; Eisenberg, Speer & Hunt, 2012; Dixon, Roberts, Lawrie, Jones & Humphreys, 2008; Chawla, Balhara & Rajesh Sagar, 2012). It is therefore essential to sensitize, educate and train medical students in all these aspects (Altindag, Yanik, Ucok, Alptekin & Ozkan, 2006; Mino, Yasuda, Tsuda & Shimodera, 2001). The first step to designing anti-stigma interventions is to identify the prevailing perceptions in specific populations. In this article, we tried to record the perceptions of a sample of medical students about two major psychiatric disorders: schizophrenia and bipolar disorder.
Our results demonstrated the need to increase efforts to provide medical students with accurate information on mental illness, especially in regard to the clinical features and effective treatment modalities for these diseases. This is an important finding, since less than half the sample were able to suggest psychiatric treatment interventions (e.g., use of oral medication, injections or hospitalization) for the patients described, even though a third of the respondents recognized the presence of mental illness in both vignettes.
The lack of knowledge of these students (and future professionals) regarding the administration of effective psychiatric treatment could be a plausible explanation for the knowledge gap that exists when psychiatric patients are under the care of general practitioners and other non-mental health professionals. To reduce this gap, medical training must include information on the services and treatments available for psychopathologies, not just the theoretical aspects regarding their definition and etiology.
Stigma towards mental illness stems from the traditional concept of danger and incompetence (Ottati, Bodenhausen & Newman, 2005), which is even more evident in the case of major psychiatric illnesses such as bipolar disorder and schizophrenia. Medical students are part of a social and cultural context which views these conditions as aggressive. In this study, we found that a significant percentage of respondents regarded the cases represented in both vignettes as potentially aggressive and, in general, made no distinction between schizophrenia and bipolar disorder. However, perceived dangerousness was more frequently considered in the schizophrenia vignette and more stigmatization was found in students who perceived aggression in the subject described in the schizophrenia vignette than in those who did not perceive it. These findings could be explained by the fact that more students only identified schizophrenia as an illness, and therefore stigma was higher in this group. Consistent with international reports (Magliano et al., 2011; Magliano, Read & Marassi, 2011), schizophrenia is the pathology most frequently thought to carry a risk of aggression. Moreover, in comparison with bipolar disorder, schizophrenia tends to be perceived as a more severe mental disorder, in addition to being less tolerated and more stigmatized (Durand-Zaleski, Scott, Rouillon & Leboyer, 2012; Stip, Caron & Mancini-Marïe, 2006).
Although the present paper might make useful contributions to the literature on stigma in schizophrenia and bipolar disorder, there are a number of limitations that should be mentioned. We are aware that the high specificity of the sample limits the generalization of our findings. First, including only students in their first year of their medical course where their knowledge about mental disorders and treatment options is limited. Future studies should include medical students from different years, and variables related to illness recognition, treatment, attitudes toward mental disorders, and perception of aggression and dangerousness should be compared between them, probably to identify changes during medical training. Second, students were recruited in just one university; it would be desirable to include students from different universities as this may provide a broader picture of the phenomenon of stigma in this particular population.
Despite these limitations, our findings reflect the need to direct efforts toward the importance of including clear and updated information about mental disorders since the beginning of the medical training. During medical school, it is important to reinforce contextualized anti-stigma programs that include the incorporation of truthful information on multi causality, clinical presentations, implications and integral treatments for such conditions in order to modify and reduce misconceptions about psychiatry and psychiatric patients. Health professionals providing attention, care and information not only to patients but also to their families and the general population should be well informed and aware of the role stigma plays as an obstacle to improving mental health care and quality of life for people with psychopathology (such as schizophrenia or bipolarity). This is particularly important in the context of the efforts that must be made to reduce the enormous treatment gap for mental disorders by increasing the identification and treatment of these problems in primary care settings.