Introduction
The suicide phenomenon is considered a public health problem at the local as well as the national level. As we know, suicide has multifactorial causes, including physical, individual, emotional, social, and environmental factors. In short, suicide cases are mainly associated with conditions such as psychosis (Overholser et al., 2018), depression, substance abuse (Underwood, et al., 2018), violence, or aggression (MacIsaac et al., 2018), and family problems. (Frey & Cerel, 2015).
Suicide behavior is a top priority among public health problems worldwide. According to the official statistics of the World Health Organization (WHO), 800,000 people commit suicide annually worldwide (WHO, 2019).
Suicide mortality has increased worldwide in both men and women, but more so in men. This male/female mortality ratio rose to over 6:1 in 1993, before falling and remaining close to 5:1 in the past decade (Borges, Orozco, Benjet, & Medina-Mora, 2010; Bertolote & Fleischmann, 2015). Suicide mortality has increased in low- to medium-income countries, as well as in high-income countries, albeit in different socio-demographic contexts. An example of this is the United States, where in 2015 nearly 100 people died by suicide every day. In fact, among Americans under 40, suicide is the second main cause of death (Miller, Azrael, & Barber, 2012).
According to the WHO (2019), in Mexico, the suicide rate is 5.1 per 100,000 inhabitants. According to Borges, Orozco et al., (2010), nationwide, suicide is one of the five leading causes of death in the Mexican population under 35. In analyses by geographical distribution, Yucatan is among the five states with the highest suicide mortality rate (Sánchez, Serrano, & Márquez, 2015).
There are studies that have addressed the phenomenon of suicide in Yucatecan society, particularly because the traditions and beliefs of Mayan culture still remain in force in this society (Hernández Ruiz, 2010). In this cultural context, suicide has positive connotations when perceived as a means of going to heaven (Villagómez, Balcázar, & Paz, 2005). However, outside the social and anthropological context, the recent epidemiology of suicide mortality in the state of Yucatan has hardly been studied.
The epidemiological approach to mortality by suicide makes it possible to understand the scope of the problem, estimate trends over time in different regions, and identify social determinants. Once a description of suicide mortality trends has been obtained, it can serve as the basis for implementing public health programs and assigning resources to implement strategies designed to influence these social determinants and design appropriate measures for the most- at-risk population. Accordingly, the objective of this study is to describe the epidemiological characteristics of people who died as a result of suicide in the period between January 2013 and December 2016.
Methods
This cross-sectional observational study included all the suicide mortality records in the databases of the Instituto Nacional de Estadística y Geografía (INEGI) produced with information from the birth and death records compiled by the Departamento de Epidemiología of the Secretaría de Salud. For the purposes of this study, suicide mortality records for 2013, 2014, 2015, and 2016 were included, since they had been obtained using the same methodology and coding, together with the most recent mortality data published by INEGI.
The diagnoses included in the death certificate and, therefore, in the mortality database, use the Tenth Revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10). For the purposes of this study, deaths with ICD codes beginning with the letters “X” and “Y”, specifically X60-X84 and Y87.0, corresponding to mortality by suicide, were included.
Annual suicide mortality rates per 100,000 inhabitants were obtained to make comparisons between states, due to the differences in the number of inhabitants and the production of annual state frequency graphs
Study variables. According to the PAHO, any epidemiological study, regardless of the pathology it addresses, considers three basic health determinants: time, place, and person. Accordingly, we have selected the variables, with their respective categories and scales, so that they are also suitable for the context of the region studied.
Sex. As a binary variable indicating whether the death corresponded to a man or a woman.
Age. Obtained using the formula (date of death-date of birth/365.25). Categories were created to identify adolescents (≤ 19 years) and older adults (≥ 65 years).
-
Marital status. Classified as married or unmarried at the time of death.
-
Residence in the state capital. The forms determine whether the deaths correspond to the municipality of the capital city (Mérida) or municipalities in the interior of the state.
-
Place of occurrence (urban). Indicates whether the self-injury occurred in an area with urbanization services, which, according to INEGI, refers to a population size of over 2,500 inhabitants. Two dichotomous variables were also generated to determine whether the death had occurred in the home or the workplace.
-
Indigenous ethnic group. In the case of Yucatan, the ethnic group is Mayan. A person was considered a member of this group when he/she (a) spoke Mayan, (b) was a resident of a town recognized as Mayan, or (c) one of his/her surnames was Mayan.
-
Educational attainment. Indicates whether the deceased studied beyond basic education, which in Mexico is equivalent to having completed middle school (Zorrilla Fierro, 2002). Educational attainment is an indicator of development related to health and has been studied in association with depression by authors such as Belló, Puentes-Rosas, Medina-Mora, & Lozano, 2005.
-
Medical care. Indicates whether a person received medical care at a health unit after self-injury and before the moment of death. A binary variable was also generated indicating whether an autopsy had been performed.
-
Employment status. Indicates whether the person was employed at the time of death.
-
Method of suicide. In accordance with the ICD-10, suicide methods are classified as drowning or suffocation, hanging, agrochemical or pesticide use, firearms, abuse of medication or illicit drugs, blunt injuries or intentional falls, smoke or gas, and injuries from sharp objects.
-
Time frame. As for the time when the suicide was committed, three eight-hour slots were established: morning, from 6 am to 2 pm; afternoon, between 2 pm and 10 pm, and finally, night from 10 pm to 6 am.
-
Month of death. Suicide acts were classified by month of mortality and the expected/observed suicide mortality ratio. This ratio was calculated for each month by dividing the total number of cases observed each month by the expected proportion of cases among the twelve months of the year = expected SM/observed SM. To estimate this, first of all, the proportion of cases observed per month was obtained. The frequency of cases observed each month was recorded, in order to obtain the proportion in relation to the total. The proportion of expected cases per month was obtained and then divided by the proportion between the twelve months comprising the annual cycle, adjusted by the number of days in each month. This measure has been used in other phenomena associated with mortality that follow a seasonal pattern.
Statistical analysis
For the descriptive statistics and the analysis of the suicide method, as well as the variables of health determinants, summary, central tendency, and dispersion measures were obtained, using hypothesis contrasting tests to identify intra- and inter-group differences by sex and injury method, in both the comparison of means for the numerical variables and the comparison of proportions for the categorical variables.
Logistic regression models were generated (for binary dependent variables), where the predefined independent variables were included one by one and preserved in keeping with the criteria of maximum likelihood and explained variance. These criteria are expressed for each model in the pseudo R2 and loglikelihood values, so that the model chosen has a pseudo R2 value closer to one and a loglikelihood closer to zero (Juul, 2006). For each suicide method, the epidemiological characteristics were contrasted, assigning a value of RR = 1.00, so that the characteristics studied that showed an RR < 1.00 had an inverse association with the injury method in question, and the characteristics with values of RR > 1.00 had a direct association. Confidence intervals were set at 95% and the alpha value at 0.05.
Results
Between 2013 and 2016, 24,964 cases of suicide mortality were registered in Mexico, together with a downward trend in the annual number of suicides. During this period, the state of Yucatan was among the five states with the greatest increase in the number of suicides. Mortality rates per one hundred thousand inhabitants for each state were plotted per year, as shown in Figure 1.

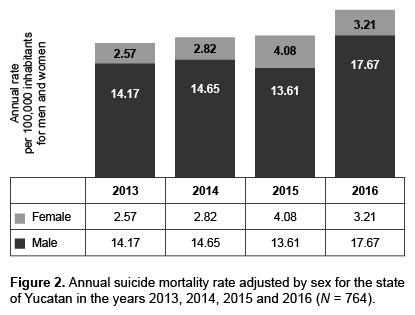
In the state of Yucatan, between 2013 and 2016, a total of 924 deaths due by suicide were recorded (Table 1), 82.2% of which were male, with a ratio of 4.6 men for every woman. The ratio of mortality by state and the difference rates by sex are given in Figure 2 .

The sociodemographic characteristics of individuals who died by suicide are shown in Table 2. It was observed that women died at younger ages than men (men 38.92, women 33.78 p = 0.001). Forty per cent of suicides were committed by people whose place of residence was Mérida (which accounts for over half the total population of the state); while 60% occurred in municipalities in rural or semi-urban areas. A total of 42.5% of the deceased had completed middle school, as opposed to 57.5% who had not. A third of those who died by suicide were married and 70.8% were indigenous people.

Over three quarters of the suicides occurred in the home and in people without formal employment. Just over a quarter of the individuals were affiliated to a public health institution and a similar proportion were taken to the health centers while still alive and received medical care before dying. Suicides occurred more frequently at night (between 10 pm and 6 am); 0.8% occurred in the workplace, and autopsies were conducted in approximately 97% of all cases.
Hanging was the most common method of self-injury, followed by agrochemical or pesticide use, which together accounted for nearly 95% of mortality cases. All the individuals who chose hanging died without medical assistance (Table 2).
Regression models identified that older adults were more likely to choose hanging (Table 3). Agrochemical mortality was 50% less frequent among those living in the capital city and the adolescent population. Agrochemical use was associated with a greater likelihood of receiving medical care before death (24.5 to 1.00) compared with the other methods.

Adolescents were more likely to use firearms as a method of suicide, which is significantly associated with death before receiving medical care. Illicit substance and drug use was more common among those who had only completed middle school. Gas poisoning was associated with residence in the capital city and was less common in males.
The monthly distribution of suicide cases is shown in Figure 3 , in which it can be observed that the month with the highest mortality rate for observed/expected suicide is May.

Discussion and conclusion
We have presented the distribution of suicide mortality in the state of Yucatan, Mexico, for the period between 2013 and 2016. The results suggest that suicide is an ongoing problem in the state, which is important to address.
The suicide mortality characteristics observed in this study showed differences in sociodemographic aspects and the factors associated with death between men and women. First of all, we have documented the fact that the male-to-female suicide mortality ratio in Yucatan was 4.6 to 1. The higher incidence of completed suicides in male sex has previously been demonstrated in various geographic and sociocultural contexts (Goñi et al., 2018; Fergusson, Woodward, & Horwood, 2000; Grøholt, Ekeberg, Wichstrøm, & Haldorsen, 1998; Gould, Fisher, Parides, Flory, & Shaffer, 1996).
According to Jokinen et al. (Jokinen, Talbäck, Feychting, Ahlbon, & Ljung, 2018), there is likely to be a convergence of several factors that make men more vulnerable to suicide than women, through four main avenues that are not mutually exclusive: a) the lack of help-seeking among men who need psychiatric help, which could be based on behaviors learned in the sociocultural context; b) the impact of socio-economic problems on men, which could be reinforced in societies where men are considered the main providers; c) the effect of the divorce and estrangement of parents, which despite the fact that this creates conflict for men and women, is unlikely to be acknowledged by men as a result of gender roles and expectations for men; and lastly d) the role of testosterone, which could contribute to the decision to commit suicide and the severity with which lethal harm is inflicted.
It should be mentioned that although suicide mortality in Yucatan was more than four times more common in males than females, in the present study we observed that women who committed suicide were younger than their male counterparts on average and that, in addition, the proportion of adolescent suicides was higher in females than males. Accordingly, it would be useful for future studies to address the underlying causes of this apparently atypical pattern, since it is only in certain Western Pacific countries that the proportion of all deaths due to suicide is higher in women than men (WHO, 2014).
Previous experimental studies have discussed the apparent need to develop preventive interventions designed specifically for either men or women, even though the evidence available in systematic reviews is not conclusive about whether they are more effective (Krysinska, Batterham, & Christensen, 2017).
As for the method of suicide, we found that hanging is the most commonly used method (87.57%), while agrochemical use (7.07%) was the second most frequently chosen method in addition to the fact that it is proportionally more common among women and older adults. Data from Yucatan on the method of choice are therefore consistent with the data reported nationally in Mexico. The most commonly used method in both sexes (81%) has been hanging, followed by shooting with firearms in men and poisoning by pesticides in women. (Sánchez et al., 2015).
Unlike those who chose hanging, individuals who poisoned themselves with agrochemicals were more likely to reach hospital alive, indicating, among other things, that training health personnel to deal with these emergencies properly is essential in our environment. Agrochemicals were chosen proportionately more frequently by women than men and by the rural population. In their research, Banerjee and Chowdhury detail the context in which, in poor countries, the dynamics of intrafamilial violence, lack of proper regulations for the safe handling of agrochemicals, and female susceptibility to exposure to toxic substances contained in agrochemicals converge in rural and agricultural environments. The tragic upshot is a widespread increase in mortality from agrochemical poisoning, which has made this a problem of public health, sanitary regulation, vulnerability, and social inequity (Vijayakumar, 2015; Banerjee & Chowdhury, 2017).
In contrast to the statistics on suicide methods reported in the present study and those documented by other authors nationwide, international data indicate that males use firearm shooting more often (Sánchez et al., 2015). As mentioned by Beautrais, Dervic, and Pompili among others, unlike the use of firearms, hanging is the most accessible method because it is economical, easy to set up and does not require meticulous planning; although it is less lethal than other methods (Beautrais, 2002; Pompili et al., 2015; Dervik et al., 2004). As for suicide mortality using firearms, it has been found that it is precisely in homes where firearms are available that this occurs most frequently. In particular, firearms are used for this purpose, not necessarily by the buyers, but by younger family members in homes where weapons are kept (Choi, DiNitto, & Marti, 2017; Miller, Warren, Hemenway, & Azrael, 2015). For this reason, WHO has suggested that reducing the access to means of committing suicide would be one way of reducing deaths (Brown, Imura, & Osterman, 2014; WHO, 2017).
Follow-up care by health personnel through regular contact, including by phone or home visits, for people who have attempted suicide, together with the provision of community support, is essential, because people who have already attempted suicide are at the greatest risk of doing so again (Berrouiguet et al., 2017).
Lastly, the monthly pattern observed in committing suicide has been previously reported in agricultural societies from different geographical areas, such as India and Russia (Cartelón, 2017). Beyond the basic knowledge involved, the importance of analyzing these seasonal patterns lies in the need to implement measures to prevent suicidal behavior with an emphasis on periods with historically higher incidence.
Suicide in the state of Yucatan is a health problem that has increased for both sexes and predominates during the month of May.
In Yucatan, men are three times more likely to commit suicide than women, yet women are proportionally more likely to commit suicide in adolescence.
Preventive measures to address this problem in the state could incorporate strategies specifically designed to address the epidemiological characteristics of the population with the highest suicide risk in Yucatan and other regions with comparable epidemiological characteristics.
Limitations. Due to its retrospective nature, the results of the present study only refer to the period studied and are therefore not intended to perform a predictive function. Since an autopsy was not performed in all cases, some deaths may have been wrongly classified as suicides.