Introduction
Having any type of cancer involves the possibility of death, accompanied by pain, loss of independence, and decreased self-esteem (Rouhani & Holland, 2003). Breast cancer is the most common oncologic pathology in women worldwide, with over two million diagnoses estimated in 2018, accounting for 11.6% of all cancers. In Mexico, the incidence of breast cancer in women has increased in recent decades, and in 2018 it ranked first with 26%, followed by thyroid cancer with 9.7%, and cervical cancer with 7.5% (GLOBOCAN, 2019).
A person’s ability to cope with a cancer diagnosis and treatment varies according to the evolution of the disease and depends on medical, psychological, and social factors such as medical care, the characteristics of the disease (clinical evolution, site of onset, type of treatment), previous level of adaptation to the condition, prognosis of the disease, management of losses suffered in one’s lifetime, emotional support, personality traits, coping mechanisms, cultural, spiritual, and religious environment, and the possibility of physical and psychological rehabilitation (Massie & Greenberg, 2019).
According to Saavedra and Villalta (2008a), resilience proposes an explanatory hypothesis of healthy behavior in adverse or high-risk conditions. It is a personal trait, constituted on the basis of the early bond and cultivated throughout the history of the subjects, enabling them to appropriate life events. For Rutter (2012), resilience can be defined as a reduced vulnerability to risk experiences, overcoming a stressor or adversity, or a relatively good outcome despite experiences of risk. It is therefore an interactive concept in which the presence of resilience must be deduced from individual variations in the outcomes of those who have experienced a significant stressor or adversity.
It is currently thought that resilience also plays an important role in the experience of adverse or traumatic events, such as disease process. The work of Grotberg (2003) in The International Resilience Project 2003-2005 proposed a resilience model based on the possession of three resources expressed as follows: “I am,” “I have,” and “I can.” Although Grotberg states that, for her conceptualization of resilience, not all the resources mentioned are required, the presence of only one of them does not suffice: in other words, resilience is the result of the combination of these three resources. These resources provide an idea of how the subject appropriates reality and opens up the possibility of a healthy behavior or overcoming traumatic events.
Based on the above, Saavedra and Villalta (2008a) take up the notion of the resources raised by Grotberg (2003) and add the history of the subject, on the assumption that the way each person interprets and acts in the face of problems recurs throughout their lifetime. Accordingly, for these authors, a resilient response is an action characterized by an evaluation of the cognitive and affective elements of the problem that arise from a system of beliefs and social ties that provide security. These authors created a resilience scale, which proved to be valid and reliable for the Chilean general population (Saavedra & Villalta, 2008b).
The interest in studying these issues stems from a repeated observation in clinical practice: women who seek oncology services - regardless of their economic, social or environmental conditions - react to and cope with the diagnosis in very different ways, which, in some cases leads to the presence of depression and/or anxiety. But what are the individual differences that lead women with breast cancer to produce maladaptive psychological responses that can lead to the development of a psychiatric diagnosis? One possible answer is resilience, which has been studied in a medically ill population because the loss of physical health is considered an adverse event in life related to psychological processes. Previous studies in other countries (Alcalde, Alcalde, & Palacios Banchero, 2011; Becoña Iglesias, 2006; Benvenuto Haase, 2015; Moscoso-Escalante & Castañeda-Chang, 2018; Retiz Flores, 2016) show that valid, and reliable resilience measurements do exist. One of the main strengths of the SV-RES scale is that it addresses the different components of resilience, rather than adopting a one-dimensional perspective, as has traditionally been the case in studies with medically ill populations using the Resilience Scale created by Connor-Davidson (CD-RISC; Connor & Davidson, 2003; Markovitz, Schrooten, Arntz, & Peters, 2015; Matzka et al., 2016; Min et al., 2013; Sharpley, Bitsika, Wootten, & Christie, 2014).
Although the SV-RES scale was created and validated in a Spanish-speaking and Latin American population, it is necessary to evaluate its psychometric characteristics to determine whether it is useful for the sample in this study and could therefore be included in the broader research of which it formed part. In this respect, Reyes-Lagunes (2011) states that when a scale has been designed in a different cultural environment, it is essential to know its structure in the new context. The objective of the present study is therefore to appreciate the different components of resilience proposed through the SV-RES Scale in a sample of Mexican women with breast cancer diagnosis.
Method
Study design
Cross-sectional, non-probabilistic study.
Participants
A sample of 114 women with breast cancer attending a specialized cancer center in the south of Mexico City was studied. The study was reviewed and approved by the ethics committee of the Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz (CEI/C/021/2015). The women were invited to voluntarily collaborate in the study. Those who agreed signed an informed consent form prior to their participation.
Participants were recruited by the principal investigator during the first clinical psychiatric evaluation and selected on the basis of the following inclusion criteria: patients with breast cancer in outpatient treatment, who were undergoing any form of cancer treatment (surgery, chemotherapy, or radiotherapy), were at any stage of the cancer process, and could read and write. Exclusion criteria included the presence of comorbid neoplasia or clinically evaluated cognitive impairment. Patients who met the inclusion criteria were invited to participate voluntarily and told the objective of the research. They were informed that their participation was independent of the care they received at the center, and that they would be able to leave the study at any time.
The procedure used to calculate the sample size was contrasting proportions (with an alpha level of 5% and statistical power of 80%), since validation of the scale was part of a broader research project in which the relationship between resilience and depression and anxiety was studied. This sample size is suitable for factor analysis (Brown, 2015), and was calculated using Stata 13.1 (StataCorp, 2014).
Measurements
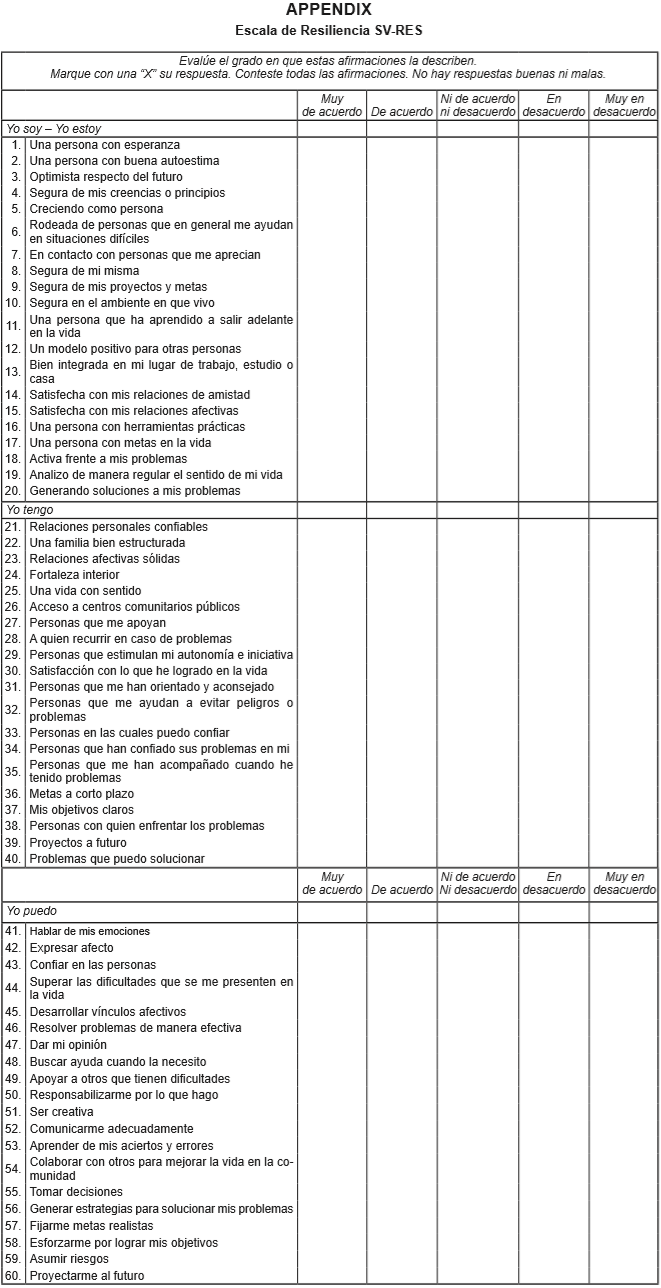
Resilience Scale (SV-RES). This scale was developed by Saavedra and Villalta in Chile and is a Latin American resilience measurement alternative designed to answer two questions: “What personal resources does the subject use to cope with adversity in a conscious, intentional way?” and “How is resilient behavior constituted from the perspective of the subject?” (Saavedra & Villalta, 2008a).
It is a self-applicable scale with 60 items divided into three resources “I am,” “I have,” and “I can,” which in turn form 12 specific resilience factors: identity, autonomy, satisfaction, pragmatism, links, networks, models, goals, affectivity, self-efficacy, learning, and generativity. The questionnaire has Likert-type response options, ranging from 1 - “strongly disagree” to 5 - “strongly agree,” yielding a minimum score of 60 and a maximum of 300 for the total scale. The highest score reflects greater skills or resilient characteristics. The validity study carried out by the authors showed a concurrent r = .76 and reliability measured through the Cronbach’s alpha of .96 (Saavedra & Villalta, 2008a).
For the purposes of this research, prior to the application of the scale, the cultural relevance of the contents of the instrument was analyzed, on an item-by-item basis, through an invitation to participate in two focus groups: one with five experts on oncology and another comprising ten women with breast cancer. Based on the observations made by the participants of both groups, some adjustments were made to clarify the contents of the items. Among the changes made, clearer, more precise language was used for women. For example, item 16, “I am a practical person” was modified to “I am a person with practical tools;” item 19 was modified from “I constantly review the meaning of my life;” to “I regularly analyze the meaning of my life;” and item 26 was modified from “I have access to social-public services” to “I have access to public community centers.”
Procedure
Eligible women candidates were identified and given the self-applicable questionnaire. Care was taken to ensure that the respondents understood the questions properly. The sociodemographic and clinical data of each participant were recorded in a database specifically designed for this purpose.
Statistical analysis
First, the sociodemographic and clinical characteristics of the study sample were reported through central tendency and dispersion measures for quantitative variables, as well as percentages for qualitative variables.
Second, the factor structure of the items was analyzed through a Exploratory Factor Analysis (Tabachnick & Fidell, 2013), using the main components method for extracting and estimating the parameters (factor loads and variances). The advantage of the principal component method is that it does not impose restrictions on the distribution of the parameters and is robust to violations of multivariate normality (Fabrigar, Wegener, MacCallum, & Strahan, 1999). The promax oblique rotation method was used rather than orthogonal rotation, since it provides a more realistic representation of the relationship between the factors (Brown, 2015). The factor structure was separately explored for each theoretical resource presented, and an exploratory factor analysis was undertaken of items 1-20 for the “I am” resource; from 21-40 for the “I have” resource, and from 41-60 for the “I can” resource. In factors with eigenvalues greater than 1, the factor loads of the items were identified, which were considered if they exceeded the .35 value and its theoretical content. Cronbach’s alpha (Streiner & Norman, 1995) was calculated as an indicator of internal consistency.
Statistical analyses were performed using SPSS software (version 21) (IBM Corporation, 2012).
Results
A total of 114 women diagnosed with breast cancer were included. The average age was 54.42 years, with an age range of 33-94 (SD 10.14 years). The average number of years of schooling of the sample was 8.44 (SD 3.78 years). Over a third of the women (36.9%) had some type of occupation involving financial remuneration, whether self-employment, part-time, or full-time, work.
Regarding the clinical variables, 56% were at an early clinical stage (in-situ cancer until clinical stage IIA) and, at the time of the evaluation, were undergoing chemotherapy-based treatment (81.6%) or surgery (69.3%).
Factor structure
Factor analysis of the resilience scale was carried out using the method of extracting principal components through oblique rotation. See, Table 1 below for the items comprising each of the three resources with their respective factor loads and internal consistencies.
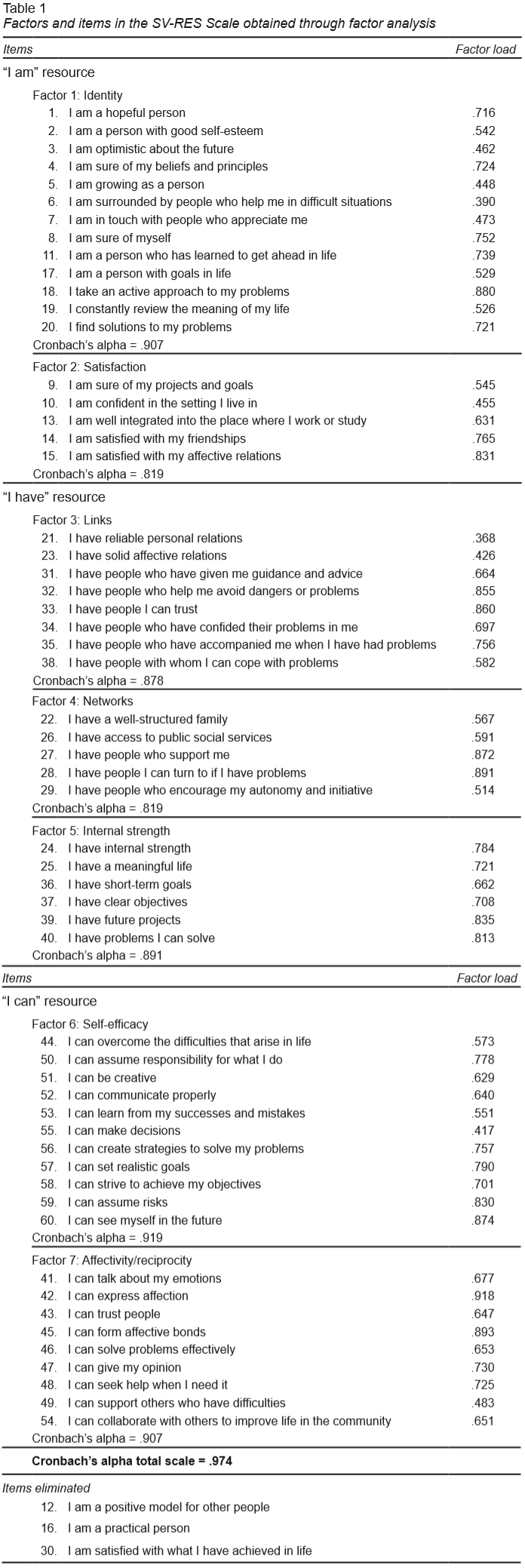
For the “I am” resource, two factors were found which together accounted for 52.52% of the variance (Table 2). Because two items loaded on both factors, it was decided to eliminate them (items 12 and 16). Factor 1 was called “Identity,” while factor 2 was called “Satisfaction.”
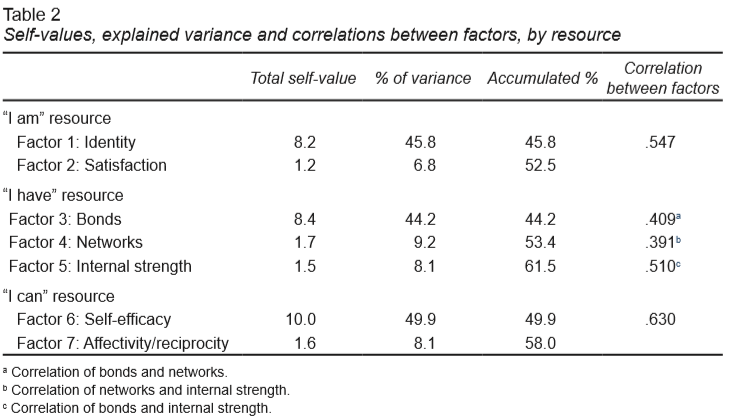
For the “I have” resource, three factors were identified that explained 61.54% of the variance; item 30 was eliminated because it loaded on all three factors. Factor 3 was called “Bonds,” factor 4 was termed “Networks,” and factor 5 was designated “Internal strength.”
Lastly, for the “I can” resource, two factors were found that together accounted for 57.97% of the variance, without eliminating any items. Factor 6 was called “Self-efficacy,” while factor 7 was termed “Affectivity/reciprocity.”
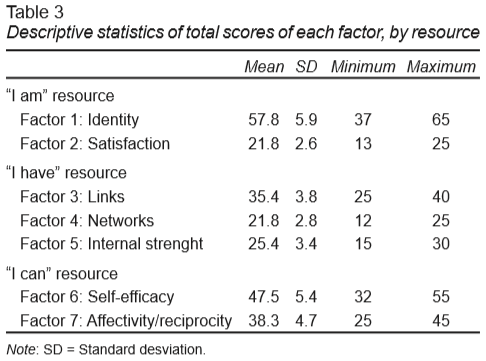
The total scale –with 57 items and seven factors– had high overall internal consistency (Cronbach’s alpha of .97) and accounted for 72.75% of variance. It is worth mentioning that although some of the factors identified coincide with those proposed by the authors of the scale, there were others that are not the same and were entitled “Internal strenght” and “Affectivity/reciprocity.” Finally, the descriptive statistics of the scores by factor are shown in Table 3.
Discussion and conclusion
The SV-RES scale is a valid, reliable instrument for assessing resilience in Mexican women with breast cancer. The overall internal consistency obtained was extremely adequate (Cronbach’s alpha = .97) and coincides with that reported by the authors of the original instrument (Cronbach’s alpha = .96) (Saavedra and Villalta, 2008a), and is similar to that obtained by Lerma et al. (2019) in Mexican patients with chronic renal failure undergoing hemodialysis (Cronbach’s alpha = .96) and higher than that reported in the Mexican Resilience Scale (Cronbach’s alpha = .93) (Camacho Valadez, 2016).
The factor structure obtained in this study was different from the original proposal, with seven factors being obtained instead of the 12 identified by the authors, which jointly explained 72.7% of the variance. These differences may be due to sociodemographic factors. For example, the original validation was carried out in the general population (men and women) aged between 15 and 65, whereas our sample consisted solely of women with oncologic pathology. We also consider that the grouping of items into certain factors may be related to their cultural understanding; for example, item 17: “I am a person with goals in life,” which was originally located within the “Pragmatism” factor is grouped under the “Identity” category here.
The most consistent items were those related to problem solving, emotional ties and future projection. These results were consistent with similar research on breast cancer patients. For example, Ocampo et al. (2011) showed a positive, significant correlation between breast cancer patients and the dimensions of social support, strength, meaning of life, and identity. There is also evidence to suggest that individuals with greater resilience have certain characteristics such as adequate reality checks, greater tolerance of negative emotions, a strong capacity for self-reflection, and a great sense of responsibility (Vanderpol, 2002), essential to understanding the emotional response to the disease and its treatments.
As a self-applicable instrument with adequate reliability for clinical practice and research on the oncological population, it is useful for determining the psychological resources women have such as resilience.
A limitation of the present study is that the cultural adaptation of the items in the SV-RES scale was not carried out in the general Mexican population, but with two focus groups: one with experts in oncology and the other comprising women with breast cancer. Another limitation is related to the selection of participants, which was based on a non-probabilistic sample of women attending a specialized care center in the south of Mexico City. Lastly, although the sample obtained was enough to conduct the exploratory analysis, it was not possible to obtain the confirmatory analysis due to the limitations indicated by the Green (1991) model, which remains pending for future research.
These findings should be viewed with caution before extrapolating them to all Mexican women with breast cancer. However, educational attainment and the proportion of women with paid work in our study sample are similar to that of the national population (42.2%) (Instituto Nacional de Estadística Geografía e Informática [INEGI], 2019; Organización Internacional del Trabajo, 2014; Secretaría del Trabajo y Previsión Social, 2019).
Regarding future implications for resilience research, it is essential to identify the factors that will make it possible to homologate its conceptual definition and standardize evaluation measures - even longitudinally. Likewise, it is necessary to promote research on resilience and its impact on the health-disease process, as well as the development of care programs that promote resilience as a means of contributing to a more comprehensive management of medical conditions, to improve well-being and quality of life for all individuals.
This is important when considering the clinical implications in which, through a greater knowledge of psychological processes in this group of patients, care programs that promote positive psychology can be implemented –with special emphasis on resilience– to reduce the emotional burden and psychiatric diagnoses and thereby improve the quality of life in women with breast cancer.